Scientific and clinical medical problems to deal/work with
Dear reader, the below may be heavy for those not familiar with scientific issues. Sorry, below is not very easy to read. Will try to do a more readable/understandable version soon – while this is what concern all of us, whether we realize it or not!
First, in brief;
Science (e.g. medicine) levels purposes are
(a) focus on knowledge development clarifying paradigm, hypothesis etc. (at best based on Popper´s three worlds approach (Popper’s three worlds – Wikipedia) and evolution of man in biopsychosocial-cultural real world), which are subjected to
(b) empirical focus to hypothesis testing in terms of falsifying data (nomothetical and ideographic, at best, systems integrating paradigm), where technology and methodology prevent addressing many very much needed fields, e.g. lifestyle related medical diseases and mental problems – so far and
Clinical levels are to empathically encounter, communicate pedagogically, encourage, educate, guide and validate individuals (ideographic paradigm).
But science levels have often the power to decide what clinical levels may and may not do – decide the rules/framework!
But no one – scientist or clinician or … has access to absolute knowledge (see http://biopsychosocialmedicine.com/news/how-to-deal-with-not-absolut-knowledge-which-no-one-of-us-have-access-to/
Is this “order” what we – individuals, patients or not – approve?
My mission here is to knowledge based and practical show how both levels can be integrated – in a both winner manner! Impossible? Perhaps – but I do not really know – yet!
Scientific problems
Scientific paradigmatic knowledge and methodological problems in human medicine systems?
Below I will discuss a critical “factor” which prevent development/improvement/ … in human medicine systems. As this is extremely complex, I will in footnotes, briefly describe what a base my arguments on. I am sorry not yet able to formulate myself in easy, pedagogical understood words for those the below I new for. But as my critical argument are considerable as well as my suggestion for solutions, my text below will not make any substantial contribution to a huge problem perhaps first now reveal by the Avalanche-like knowledge development within many different areas, as e.g. the cancer field!
I will try to express myself as practical as I can, but first some basics scientific and clinical problems!
Human medicine science is not platformed on absolute knowledge (NB! This text is also not resting on absolute knowledge as well – also, I do not here discuss other scientific areas concerning levels of knowledge) and therefore actual general knowledge level rests on what has been called paradigm (see Kuhn´s Cycle2), which “filters” what knowledge and its consequences are accepted.
Importantly, we need to have some kind of consensus about what and how we understand a functional approach for e.g. biopsychosocial (lifestyle) medicine (that is, what is paradigmatic accepted basics and its implications/applications for clinical and educational/coaching practice) as well as possible deal with personal thinking/work on concerning consequences of varying degree of uncertainty (and limited knowledge) – that is, expressed at individual levels level of understanding of the accepted paradigm.
This means limitations at both nomothetic (understood here as general) and ideographic (individual) levels. The above indicate that it is individuals in power positions who decide what is the norm based on their own limited knowledge (need here, for clarifying more, to introduce both a few words on George Kelly´s2 work as well as Karl Popper´s3 world hypothesis) – our general limited knowledge base.
Sound people in power positions either (a) understand they are basing their thinking/decisions/actions on a limited data base as well as their own competence limitations and thereby do the best they can realizing this as well as modestly/humbled/ reasonably acceptably act in accordance with it or (b) do not understand the above or (c) understand and miss use it for personal use purpose/manipulation/benefit – intentionally or not (see more below about “mammalian brain dominant thinking and human brain dominant thinking” 4).
Human medicine needs a reasonable satisfying functional knowledge base and guidelines how to put it into practice as well as educational systems providing competent practicing people at different needed positions.
As human intelligence, (so far) is different from computer “intelligence” concerning elaborating uncertain information, we may to some degree deal with limited knowledge discussed above, given we do not believe we base our work on absolute knowledge. It is not black or white. If we base our thinking/work on realizing limitations we can based on our educated competence with confidence (not Besser-wiser trapped) do our best with an open reasonable open mind observing what may be out of “paradigm steady state”. More is not possible. To constantly questioning are doings interfere our competence skills.
Legal framework and regulations are a must but on the other hand, some pronounced changes may overturn the whole system. But how to change the paradigm from reductionistic (but which so far in wain have been trying to approach) to systems integrating biopsychosocial medicine is something we should have been starting up since long and today seems overbearing difficult.
But, on the other hand, this is what always (?) most clinicians have worked for, called evidences based practice – but based on scientific medicine mostly approved reductionism with exceptions as by textbook by Guyton and others.
One solution is to turn upside down the power balance and increase the importance of clinical experiences and thereby also make priority for “a priori predicted repeated measurement single case design thinking” where assessment lead to pretests diagnosis hypothesis with a priori predictions and the predicted treatment process in individuals/patients are followed modified when needed finished by pos-tests as well as documentations where data is using AI-tools is move “upwards” towards subgroups papulations providing guidelines over time for new patients entering the assessment positions. Furthermore, probably may also prevention medicine will benefit from such informative databases!
Discussions; can the above be accomplished? Given people in power positions basically accept and see a paradigm change as needed, AI-tools can be used to built in in a “learning while doing” way some of the needed educational changes, if move back and forth between (first) practice to knowledge abstractions (theory) according to a plan which can integrated present needs tailored into a gradually paradigm shift.
I realize some of the problems (which can be seen as impossible to accomplish) and I do think a few fields must be “first out” to test in small groups.
One group I think will be not very difficult is hypertension if an applied psychophysiological knowledge base is added. Here nurses educated in clinical psychophysiological behavioral medicine can be coordinating between traditional medicine and patients, who here become a resource (see e.g. as an example from cancer – http://biopsychosocialmedicine.com/projects/rd-international-projects-2/placebo-rd/the-cancer-patient-as-an-educated-resource-an-coworker-in-own-rehab/)
But perhaps to easiest general way to approach a systems integrating biopsychosocial medicine is to center around the patient, somewhat in terms of the above but more wide than only (but I see it as a necessary part) psychophysiological behavioral medicine and use our or others biopsychosocial medicine toolbox; education, tailoring and actions, guided by the coordinator – based on a practice – knowledge (that order) based educated coordinator which can via practical education of guidance of patients open “the door”, given a ideographic single case design flexible real world procedure is the base for reliability and validity, including ecological, but perhaps not always possible to add integrated biofeedback during the treatment process (but if patients capacity to psychophysiologically relax e.g. control of autonomy nervous system behaviors/activities, is an useful instrument by many reasons, where patient motivation is one, documentation another.
The above means that clinical practice and ideographic based science need to go hand in hand! At the same time understanding of complex interactions between and within systems over different individual, situations and time make is hard to understand, not only what systems are interacting but the consequences, e.g. in relaxed breathing buffering systems works according other time scales than measures of etCO2, which in turn is to a large extent controlling SpO2. As breathing exercise nowadays is used often when training patient (and other to relax), we need in clinical setting measure such processes, especially as we become more and more aware of the metabolism (and mitochondria health as well) importance for most diseases and mental problem. Not just for relaxation (and influence on autonomic activities) but also for cell metabolism at large.
1 http://www.thwink.org/sustain/glossary/KuhnCycle.htm
2 Kelly’s theory of personal constructs. George Kelly proposes that there is an objective reality, but that we cannot know it because we must view it through our personal interpretation or construction of it. His theory is expressed in a basic postulate and extended through eleven corollaries.
3 Karl Popper
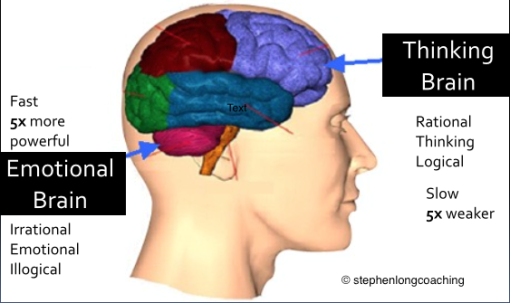
4 “Mammalian brain dominant thinking and human brain dominant thinking” is a perhaps too provoking formulation of preverbal/precognitive/spatial information processing which integrate tribune brain (https://en.wikipedia.org/wiki/Triune_brain) with dual code theory (https://en.wikipedia.org/wiki/Dual-coding_theory) and George Kelly´s personal construct theory (1955) as well as Thomas Kuhn´s paradigm and Karl Popper´s World hypothesis) … and many others not to forget Aristoteles fundaments. In brief, Limbic information processing dominate (also addressed e.g. with “emotional brain” proposals, e.g. by Joseph e. Ledoux)
Stephen Long´s picture below is very simplified but principally rough what signify difference between mammalian (part of older evolutionary part of our Limbic systems, called in man) and human brain (very recent, new evolutionary part of our brain).
 (Suggested other pictures and explanatory texts of the above are appreciated)
(Suggested other pictures and explanatory texts of the above are appreciated)
George Kelly´s “man as a scientist’s” metaphor is basically what I based my dissertation on but he also considered to use reconstructions (may connect to today’s expression reconsolidation, e.g. Karim Nader) to get free from one own´s biographic based slavery as indicated in the picture below as well as in my (1983) slogan logo for our version of stress medicine –